A client kept having flare ups. We’d tried backing off certain movements, adjusted his load, took things easier for a stretch. Nothing worked. The flare ups kept coming back and we couldn’t figure out why.
So we did something different. Took a photo from straight on and drew a line from the middle of his feet up through his body.
He was shifted almost entirely to the right. And forward. His mobility had gotten noticeably worse since we started working together, especially on the left side. Neither of us had caught it because it happened the way these things always happen: gradually, until it wasn’t gradual anymore.
This is more common than most people realize. And it’s more fixable than most people expect.
You Were Never Perfectly Even To Begin With
Here’s the thing nobody tells you: your body being asymmetrical isn’t a design flaw. It’s the design.
Your organs aren’t symmetrical. Your liver sits on the right, your heart on the left. Nobody walks around panicking about that. But the second one shoulder feels tighter than the other, suddenly it’s a structural emergency requiring six months of PT and a foam roller that cost more than your first car.
Research on postural mechanics shows humans have a natural right-side dominant bias baked into how we move, breathe, and load. The two sides of your nervous system, your respiratory system, and your hips all have different jobs and different demands on them. That’s not a malfunction. That’s how you were built.
Add thirty years of reaching, carrying, lifting, and rotating with your dominant hand and that bias gets more pronounced. You sit the same way every day. You carry groceries on the same side. You sleep on the same shoulder. You’ve been doing the same handful of movements in the same direction for decades. Your body adapted. It got really good at one version of itself.
That’s still not a problem. Until it is.
When the Body Overcorrects
The issue isn’t the asymmetry. The issue is when it gets extreme enough that your body starts treating normal movement like a threat.
When that happens, your nervous system does what it always does. It protects you. Shifts your weight, tightens things down, limits your range. All of it meant to keep you safe. The problem is when it kicks in and there’s nothing to actually protect you from. Now you’re stuck in full defensive mode with pain and no real villain to blame it on. Your body is guarding a house that isn’t on fire.
That’s exactly what was happening with my client. His body had drifted so far to one side that normal movement on the left had become restricted enough to feel threatening. The flare ups weren’t random. They were completely predictable, once we understood what was going on.
We don’t know exactly what started it. Could have been stress. A new activity. A few months of sitting differently. These things rarely have one clean cause. But once we saw the pattern, we knew what to work on.
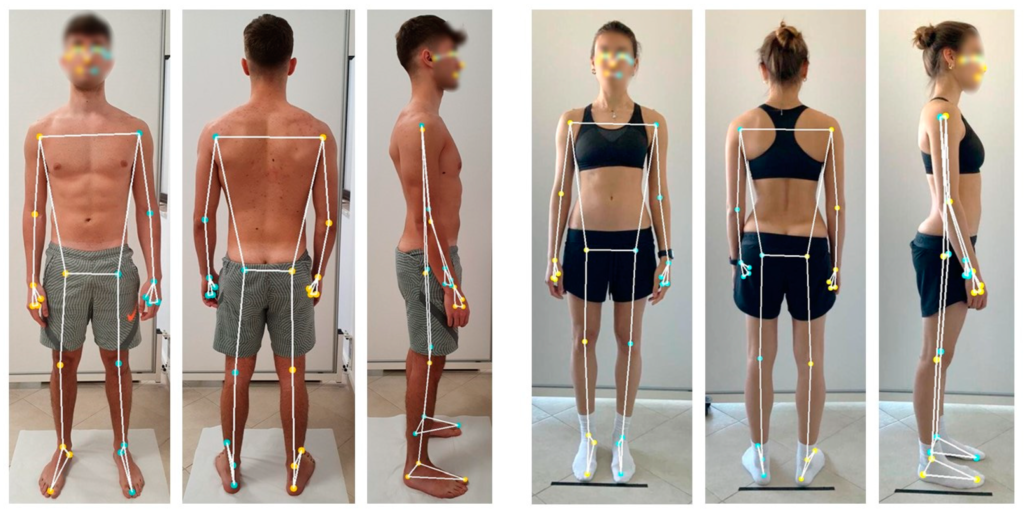
[Photo: posture assessment photo with line drawn up from feet, or simple diagram of lateral shift]
The Second Client: When Surgery Fixes the Pain But Not the Pattern
This one is worth telling separately because it comes up more than you’d think.
A woman came in after hip surgery. The surgery had gone well. The pain that had been there before was gone. But something still felt off. One side felt weaker, less connected, harder to trust. Day to day she just felt crooked.
We did the same assessment. Drew the line from the middle of her feet up.
She was shifting her weight away from the surgical hip. The pain was gone but her body hadn’t gotten the memo. It was still in protection mode, still treating the hip like it was broken even though the thing that was broken had been fixed months ago. Turns out your nervous system doesn’t automatically update when the surgical report does.
Her rehab had addressed the surgical site. It hadn’t addressed the compensatory pattern her body had built up around it.
We started with mobility work to open up that side. But before any of that, we did something that sounds almost too simple to work. She lay on her side with her feet against the wall, just letting her foot make contact with the wall, and breathed. That’s it. No reps, no load, no complicated cueing. Just giving her nervous system a chance to feel that side again, to register that the foot was there, that the hip was there, that it was safe to be on that side.
It sounds like something you’d see in a relaxation video. It works because your brain needs input before it can accept output. You can’t strengthen a side your nervous system has decided to ignore. You have to reintroduce it first.
From there we layered in mobility work and made sure her strength training kept her aligned and loading evenly rather than defaulting back to the pattern she’d been stuck in. Over a few weeks the shift corrected. She stopped feeling off. The side that had felt disconnected started feeling like hers again.
Strength Asymmetry Is a Different Problem
These two things get lumped together constantly and they shouldn’t.
Strength differences between sides are almost always normal and almost always not worth stressing about. If one arm is stronger than the other, that’s handedness doing what it does. Research shows side-to-side strength differences of up to 10-15% are within the typical range for most people.
In sports that favor one side heavily, those differences can get much more dramatic without any issues at all. Studies on professional tennis players show dominant arm muscle volume can be over 13% greater than the non-dominant side. Rafael Nadal’s dominant arm is visibly larger than his other one. You can tell from a regular distance. That asymmetry helped him win 22 Grand Slams. Nobody pulled him aside and said his arms needed to match before he could compete.
A baseball pitcher’s throwing arm will look different from their other arm. A soccer player’s dominant leg will be stronger. That’s sport-specific adaptation. It’s the point, not the problem.
Where it matters is mobility. A significant restriction in range of motion on one side compared to the other is what starts changing how you load, how you move, and eventually how you feel. That’s the one worth addressing.
[Photo: simple side by side shoulder raise or hip hinge comparison showing range of motion difference]
Does Yours Actually Need to Be Fixed
Honest answer: not always.
If you’re not in pain and nothing feels off, leave it alone. Asymmetry alone is not a diagnosis. It doesn’t need to be treated just because it exists. Most people reading this have some degree of it and will go their whole lives without it ever becoming a problem. That’s a completely normal outcome.
If something does feel off, the question is whether it’s a mobility issue or a strength issue. Strength you can usually address by prioritizing single arm and single leg work and letting the weaker side catch up without the dominant side taking over. That’s often all it needs.
Mobility is where you need to be more deliberate. And if there’s a postural shift on top of the mobility restriction, the first step isn’t stretching. It’s getting your brain to accept the side it’s been avoiding. That grounding drill isn’t a warmup gimmick. It’s the starting point.
What to Actually Do
First, decide if this even needs your attention. Are you in pain, or does something consistently feel off when you move? If no to both, close this tab. You’re fine.
If something is nagging, take a photo from straight on, feet hip width apart, standing naturally. Draw a line from the middle of your feet up. Is your body centered on it? Check shoulder height and hip height. Then test the same movement on each side and see where the gap shows up.
If it’s a strength gap, focus on unilateral work and let the weaker side lead.
If it’s a mobility gap with a postural shift, start here before anything else: lie on your side on the floor, the side you feel less connected to, with your feet against a wall. Let your foot press gently into the wall. Just breathe. Exhale fully. Don’t try to do anything else. Do that for a few minutes and see if that side starts to feel more like yours. It sounds like it should not work. It usually does.
From there, mobility work specific to the restricted direction is the next step. But you can’t get there if your nervous system isn’t on board yet.
If you’ve had surgery or a significant injury and still feel off on that side, this is worth getting looked at with someone who understands movement, not just the site of the original problem.
⚡ ACTION ITEM OF THE WEEK
Do the Two-Minute Assessment. Then Try the Drill.
Take a photo from straight on, standing naturally. Draw a line from the middle of your feet up. Shifted to one side? Check shoulder height and hip height. Then test the same movement on each side and see where the gap shows up.
If you find a side that feels disconnected or less trustworthy, try this: lie on that side on the floor, feet against a wall, and just breathe. Let your foot make contact. Exhale fully. Give it two to three minutes. No reps, no stretching, just presence. See what changes.
If nothing feels off and nothing hurts, you don’t need to do any of this. Asymmetry alone isn’t the problem. Pain and restriction are.
Work With Me